Regulatory, Pricing and Reimbursement Overview
DLA Piper / Norway
An insight into regulatory, pricing and reimbursement overview in Norwegian Pharma. Prepared in association with DLA Piper, a leading law firm in Norway, this is an extract from The Pharma Legal Handbook: Norway, available to purchase here for USD 99.
1. What are the regulatory authorities with jurisdiction over drugs, biologicals, and medical devices in your country?
The Ministry of Health and Care Services (nw. Helse-og omsorgsdepartementet, “HOD”) is the legislative authority. The Norwegian Medicines Agency (nw. Statens legemiddelverk – “NoMA”), a subordinate to HOD; is the national authority vested with jurisdiction over both medicinal products and the regulation and monitoring of medical devices. NoMA also is responsible for certain aspects regarding the regulation of non-prescription drugs, such as marketing authorization/approvals, promotion etc.
The Norwegian Health Economics Administration (nw. Helseøkonomiforvaltningen, “HELFO”) decides on reimbursement for individual patients for where there is no general reimbursement or indication is not covered by general reimbursement.
2. What is the regulatory framework for the authorization, pricing, and reimbursement of drugs, biologicals, and medical devices?
a) Authorization
The Medicines Act (LOV-1992-12-04-132) and associated regulations such as the Medicines Regulation (FOR-2009-12-18-1839) set forth the main regulatory framework for the authorization of medicines. The Medicines Act and associated regulations implement the corresponding EU legislation, including Directive 2001/83/EC and Regulation 726/2004.
The regulatory framework regarding authorization of medical devices can be found in the Medical Devices Act (LOV-1995-01-12-6) and the Medical Devices Regulation (FOR-2005-12-15-1690), implementing the correspond- ing EU legislation, Directive 90/385/EC, Directive 93/42/EC and 98/79/EC.
The abovementioned Medical Devices Regulation will be replaced by two new EU regulations; Regulation (EU) 2017/745 on medical devices and Regulation (EU) 207/746 on in vitro diagnostic medical devices. Since Norway is not a part of the EU (only a member of the EEA) these regulations are not automatically applicable in Norway, and have to be implemented through legislative acts. The Act is expected to be finally decided by parliament spring 2020.
b) Pricing
All registered, prescription-only medicines for humans must have a maxi- mum price, set by NoMA before they can be marketed in Norway, pursuant to chapter 12 of the Medicines Regulation. The market authorization-holder (“MAH”) must apply for a maximum price. The maximum price consists of two elements; maximum pharmacy purchase price (“PPP”) and maximum pharmacy retail price (“PRP”). The PPP is decided based on several factors:
- International price comparisons. Prices in other EEA countries save as the main basis for determining the PPP. The price in other EEA countries is set as the mean of the three lowest market prices of in a selection of relevant EEA countries. The current reference countries are: Sweden, Finland, Denmark, Germany, UK, Netherlands, Austria, Belgium and Ireland.
- Price of comparable medicines including biosimilars and generics
- Production costs can be taken into consideration in special cases
The MAH and NoMA can initiate a reevaluation of the of the maximum prices. Adjustments should not occur more frequently than once per year.
PRP is decided by adding PPP and a maximal profit for the pharmacy. The maximal profit for prescription drugs are based on the following criteria as per 1 July 2019
- 2.0% add-on from the PPP
- NOK 29.00 add-on per package
- 0.5% add-on from the PPP if the prescription medicine requires cooling
- NOK 19.00 add-on per package for A/B-preparations A and B preparations are medicines that are addictive, and thus requires specific prescriptions and personal ID prior to issuing. A preparations are the strongest, and includes morphine and other opiates. B preparations are addictive and includes e.g. valium and sleeping pills.
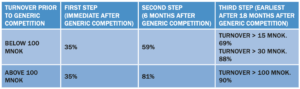
In addition, after the patent protection and, if applicable, supplementary protection certificates has expired, medicines are subject to a so called “price step model” price reduction. The purpose is to reduce the cost of pharmaceuticals. The “price step model” entails that the priced is reduced by a percentage of the original medicines maximal PPP. The PPP is reduced in two or three steps. The first step commence when there is generic competition on the market, while the second commence six months later. The third step commence earliest 12 months after commencement of the second step. The size of the price reduction depends on whether the original drug had an annual turnover of above 100 000 000 in a 12 month period within the two years prior to generic competition. The following table illustrates the “price step model”:
Prices of non-prescription drugs and medical devices are generally set without restrictions.
In order to be listed on the Blue Prescription reimbursement scheme, the manufacturer (or importer) of medical devices has to file application to HELFO, (see question 2 c below). As a part of the application process the manufacturer and HELFO agrees on a max net reimbursement price for the product in question.
c) Reimbursement
In Norway, prescription medicines are financed by the government through:
- Blue prescriptions: the reimbursable prescription regime,
- H-prescriptions: regional health authorities and medicines used in hospitals, or
- White prescriptions: by the patients through out-of-pocket payments from the patients .
The Blue Prescription Regulation (FOR-2007-06-28-814) entails that the Government, through the National Insurance Scheme, covers large portions of the costs of medicines, medical supplies such as medical devices, necessary for the treatment of serious illnesses or other risk factors that are likely to cause or intensify serious illness and where there is a need or risk of recurring treatment over a prolonged time.
Pursuant to the Blue Prescription Regulation section 2 some medicines for specific treatments are pre-approved for reimbursements. These can be found on the reimbursement list. Medicines that are not pre-approved for reimbursements, can be reimbursed based on individual application and only for long term treatment, cf. the Blue Prescription Regulation section 3. In addition medicines used to treat serious contagious diseases can be reimbursed under the Blue Prescription Regulation. HELFO covers 61% of the costs of medicines under the Blue Prescription regime, and the patient 39%, except in the case of contagious diseases and some other limited exceptions where the reimbursement is 100%.
Some medical devices for certain diseases are also covered by the Blue Prescription scheme, cf. the Blue Prescription Regulation section 5. HELFO updates a list of medical devices covered at least four times a year. It is the supplier of the medical device in question that applies to HELFO to have their product listed under the Blue Prescription Scheme.
The regional health authorities (hospitals) may reimburse 100% of costs of prescriptions for very expensive medicines intended for long term treatment (H-prescriptions). Examples of diseases where prescription drugs can be covered by H-prescriptions are Crohns Disease, Bechterevs Disease and some cancer treatments.
White prescriptions are usually paid by the patient itself. In some limited situations the state may reimburse costs for this category of medicines, such as medicines for IVF-treatments and contraceptives for women between 16 and 22 years.
In addition there is a maximum cost scheme, which entails that if a patient has reached the maximum cost within the calendar year, any additional out-of-pocket expenses from the are reimbursed by the National Insurance Scheme. There are two threshold groups; maximum cost 1 (NOK 2460 in 2020) and maximum cost 2 (NOK 2176 in 2020).
- Maximum cost 1 covers expenses from:
- Physicians visits
- Psychologists
- Hospitals
- Patient travels
- X-rays
- Medicines, foodstuffs and medical devices covered by the blue prescription scheme
- Maximum cost 2 covers expenses from:
- Treatment at physiotherapists
- Some types of dental care
- Stay at authorized rehabilitation clinics
- Treatment travels abroad organized by Oslo University Hospital
3. What are the steps to obtaining authorization to develop, test, and market a product?
a) Medicinal Products
New medicinal products must undergo an evaluation of their quality, safety and efficiency prior to being placed on the Norwegian market. The process is mainly regulated by the Medicines Regulation and the Norwegian Regulation on clinical trials of medicinal products for human use (FOR 2009- 10-30-1321), which incorporates Directive 2001/20/EC. Regulation (EU) No 536/2014 on clinical trials on medicinal products for human use, which will repealing Directive 2001/20/EC has been implemented in Norway in Regulation (2017-01-12-36) which is in turn is implemented in the Medicines Regulation (Section 15-6a) but this section has not yet entered into force. The process is monitored by NoMA.
The main steps are the following:
- Pre-clinical tests: Not regulated under the medicinal product regulatory framework.
- Clinical trials: The investigational medicinal product is tested on human beings. This is subject to regulatory and ethical review in accordance with the procedures of clinical trials in Regulation on clinical trials of medicinal products for human use
- Marketing authorization application: Once the clinical trial is finished; i.e. the pharmaceutical company has gathered sufficient data regarding the medicinal products quality, safety and efficiency it can include all the relevant data and use this to file an application for a marketing authorization/approval (“MA”) to either NoMA or the European Medicines Agency (“EMA”)
The pharmaceutical company can put the medicinal product on the market once it (1) has obtained a MA from either NoMA or EMA and (2), if a prescription-only medicine; a PPP and PRP has been set.
b) Medical Devices
A prior authorization from NoMA is not necessary before putting medical devices on the market in Norway. The manufacturer is responsible for ensuring that the medical devices is complaint with the requirements of the relevant regulation, i.e. the Medical Devices Act and the Medical Devices Regulation.
All medical devices require a CE mark to be placed on the Norwegian marked. In order to affix a CE mark, the manufacturer must conduct a conformity assessment. For Class 1 devices, the manufacturer drafts a CE declaration of conformity after having verified compliance with the applicable requirements. For Class Is (sterile), Im (measuring device), IIa, IIb, or III devices, the manufacturer must involve a Notified Body; a private legal entity designated by NoMA to exercise conformity assessment procedures. It is the Notified Body who issues the declaration of conformity required for the manufacturer to affix the CE mark.
If the manufacturer (or EU/EEA authorized representative) is established in Norway, it must register the medical device in the Norwegian Register for medical devices.
4. What are the approximate fees for each authorization?
The fees for applying for an MA of a medicinal product varies depending on the procedure, the type of medicinal product, presentation and other factors. The fees are available on NoMA’s website, and the current price for some relevant categories (per 1 January 2020):
- 422 707 NOK (37 100 EUR per 4 May 2020)for national applications for complete dossier/well established use/fixed combinations
- 105 677 NOK (9 300 EUR per 4 May 2020)) for DCP (Decentralized Procedure) application where Norway is CMS (Concerned Member State)
- 105 677 NOK ( 9 300 EUR per 4 May 2020) for MRP (Mutual Recognition Procedures) where Norway is CMS.
In addition MAHs are also liable to pay a supplier tax of 1.0% annual turnover. We recommend visiting NoMA’s website for a full list over regulatory fees and supplier taxes, available here.
5. For how long are marketing authorizations/registrations valid? How are marketing authorizations/registrations renewed?
a) Medicinal Products
The initial MA for a medicinal product has a duration of 5 years. Once renewed after the initial 5 year period, the marketing authorization is valid for an unlimited time period unless NoMA, on justified grounds, requires one additional five-year renewal period.
The renewal application should contain a consolidated version of the dossier filed with the original application, in order to enable a new assessment of risk/benefit for the medicinal product. The renewal application shall be submitted to NoMA latest 9 months prior to the end of the five year period. The renewal application can also be submitted earlier than 9 months after agreement with NoMA.
b) Medical Devices
For medical devices, once the manufacturer has obtained the CE mark, and if the manufacturer (or EU/EEA authorized representative) has registered the device in the Norwegian Register for medical devices, the device can be placed on the market, without restrictions. However, the declaration of conformity issued by the Notified Body for the CE mark has a maximum duration of 5 years, but can be renewed for additional 5 years periods.
6. How does the authorization process differ between brandname products and generic products? Are there differences for local manufacturers versus foreign-owned manufacturers?
Original medicinal products must be approved through full applications. Full applications requires the market authorization holder to submit full pre-clinical test and clinical trial data (complete dossiers).
A company may obtain MA for generic medicinal products through a simplified procedure, pursuant to the Medicines Regulation section 3-9. The applicant may document that the medicinal product is of the same qualitative and quantitative composition and the same pharmaceutical form of a reference medicinal product that has a MA within the EEA. The application can first be filed 8 years after the reference medicinal product obtained MA within EU/EEA, and the generic product may first be placed on the market 10 years after the reference medicinal product’s MA cf. The Medicines Regulation section 3-10 to 3-11.
For medicinal products that are similar to a reference medicinal product, but cannot meet the criteria of “generic” due to differences in raw materials or in production process (“biosimilars”), it is necessary to conduct comparative quality studies, comparative non-clinical studies and comparative clinical studies.
The procedure to obtain MA does not differ between Norwegian and foreign applicants.
7. How are combination products (drug + drug, drug + biologic, drug + device, biologic + device, drug + biologic + device) regulated?
Pursuant to the Medicines Regulation section 3-13, medicines consisting of combinations of active ingredients that already is used in medicines with MA, only need to submit pre-clinical and clinical data for combination of active ingredients, not for the individual active ingredient.
Combination of medicines and medical devices may be regulated either as a medicinal product or as medicinal products and a medical device. This assessment must be performed on a case-by-case basis.
NoMA can offer guidance on the matter, but also refers to the European Commission guidelines available here.
8. How is compliance with regulations monitored and evaluated? Is the regulatory regime comparable with the U.S. Food and Drug Administration or the European Medicines Agency expectations and requirements?
NoMA is responsible of monitoring compliance with the applicable rules and regulations. NoMA may also conduct site inspection and require samples of medicines. See also Marketing, Manufacturing, Packaging & Labeling, Advertising, question 11. The regulatory regime is in line and compliant with European Medicines Agency expectations and requirements.
9. What is the potential range of penalties for noncompliance?
NoMA has broad enforcement powers and may issue administrative fines, as well as revoke and suspend MAs and/or licenses.
10. Is there a national healthcare system? If so, how is it administered and funded?
The Norwegian healthcare system is founded on principles of universal access, decentralization and free choice of provider.
The healthcare system is financed by taxation, together with employer contributions and out-of-pocket payments from patients (co-payment). All residents (if a persons intended stay is for at least 12 months) or people working Norway are as a general rule mandatory members of the National Insurance Scheme (nw. folketrygden). The National Insurance Scheme is managed by the HELFO.
The provision of primary health care is decentralized at municipal level, while specialist care is managed centrally. Most hospitals in Norway are public. The small number of privately owned hospitals are for the most part funded publicly.
There is limited private medical insurance.
11. How does the government (or public) healthcare system function with private sector healthcare?
As mentioned above [Question 10], a fundamental principle of the Norwegian healthcare system is the free choice of provider.
12. Are prices of drugs and devices regulated and, if so, how?
See above, [Question 2 b) and c)] for further elaboration on the pricing and reimbursement of drugs and medical devices in Norway.
13. How are the drugs and devices used by patients paid for? What roles do public and private payers play?
In Norway, prescription medicines are financed by the government (which again is financed through taxation) through the reimbursable prescription regime (blue prescriptions), regional health authorities (H-prescriptions and medicines used in hospitals), or by the patients through out-of-pocket payments from the patients (white prescriptions). See above [Question 2 c)] for further elaboration on this matter.
14. Who dispenses drugs and devices to patients and how are those dispensers compensated?
a) Medicinal Products
Prescription drugs may only be dispensed to patients after a prescription by a physician, and can only be dispensed by pharmacies (where also online order is possible), but not by LUA distributors (i.e. medicines sold outside of pharmacies).
The contingency storage of wholesalers shall correspond to two months of ordinary sales and will be in addition to the warehouse the wholesaler would otherwise have had. The wholesaler’s cost of storage is offset by raising the maximum purchase price for pharmacies by 1% for the drugs in question from the same date. The requirement is included in the Regulation on wholesale business with medicines (FOR-1993-12-21-1219), cf. Section 5.
b) Medical Devices
Distribution by Professionals
When importing medical equipment for professional use, there is therefore a requirement that the equipment is CE marked, has Norwegian labeling and Norwegian instructions for use, and be registered in the Norwegian equipment register. In addition For more detailed information on importing goods in general, see the Customs website.
In addition to Norwegian producers, any Norwegian responsible representative, i.e. every natural or legal person established in the EEA area and explicitly designated by the manufacturer located outside the EEA area, acting on behalf of the manufacturer and can be contacted by authorities and agencies within the EEA in respect of the manufacturer’s obligations under the regulations on medical devices responsible for registration. Any natural or legal person assembling equipment bearing the CE mark has a duty to register in the equipment register is described in the Regulations on Medical Devices Section 2-8 and the Act on Medical Devices Section 10.
For Personal Use
The Medical Devices Act and the Medical Devices Regulations apply to anyone who manufactures, markets or markets equipment for use in Norway. Therefore, when importing medical equipment for personal use there will be no requirement that the equipment be CE marked, have Norwegian labeling or Norwegian instruction manual.
When purchasing medical equipment that does not comply with the regulations, the person who has purchased / imported the equipment may risk that Customs stops the shipment and that the content is either destroyed or sent back to the sender.
Free Samples
There are no specific Norwegian regulations regarding the delivery of free samples for medical devices. The basic requirements for free samples are similar to those for other medical devices. Medical devices that meet the requirements of the regulations must be affixed to the CE marking and can then be freely marketed within the EEA / EU. Labeling and instructions for free samples must be in Norwegian, similar to other equipment.
15. What are the professional and legal responsibilities of those who dispense drugs and devices? What role do they play in providing patient care, information, and safety?
All Health Care Personnel (“HCP”)’s, including physicians and pharmacists has a general duty to provide their services, such as the dispensing of drugs and medical devices, in accordance with the requirements for professional prudence and caring assistance that can be expected based on their qualifications, the nature of their work, and the situation at large, cf. the Healthcare Personnel Act (LOV-1999-07-02-64) section 4.
When HCP’s dispense drugs and devices they are obligated to give the patient sufficient information about the drug or device so that the patient can use the drug or device correctly, cf. the Pharmacy Act (LOV 2000-06-02- 39) section 6-5 with reference to distribution from pharmacies.
Also in pharmacies there is an “information duty” with respect to information provided on distributed medicine, cf. Regulation on pharmacies section 40 and section 42 if sold online.
For distributors outside of pharmacies they must not give any “medical advice” orally and must if asked always refer the question to a physician or pharmacy, cf. (“LUA”) (Nw. Legemiddel utenfor apotek) regulation (FOR- 2003-08-14-105) Section 12.
If there are several drugs available that are considered equivalent (e.g. generics or biosimilars), pharmacists and physicians must inform the patient about the alternatives and the price.